

Abstract
Introduction: Bosutinib is approved for newly diagnosed chronic phase (CP) chronic myeloid leukemia (CML) and CML resistant or intolerant to prior therapy. Efficacy and safety of first-line bosutinib and imatinib were assessed in older vs younger patients in the ongoing phase 3 BFORE trial (NCT02130557).
Methods: In all, 536 patients were randomized 1:1 to receive bosutinib or imatinib (400 mg once daily). We compared outcomes in patients aged ≥65 years (older group) vs <65 years (younger group) after 24 months of follow-up. Efficacy (excluding complete cytogenetic response [CCyR]) was assessed in the intent-to-treat (ITT) population (Philadelphia chromosome-positive [Ph+] and negative patients) of both age groups and safety in patients who received ≥1 dose of study drug. CCyR was assessed in the modified ITT population (Ph+ patients with e13a2/e14a2 transcripts [N=487]).
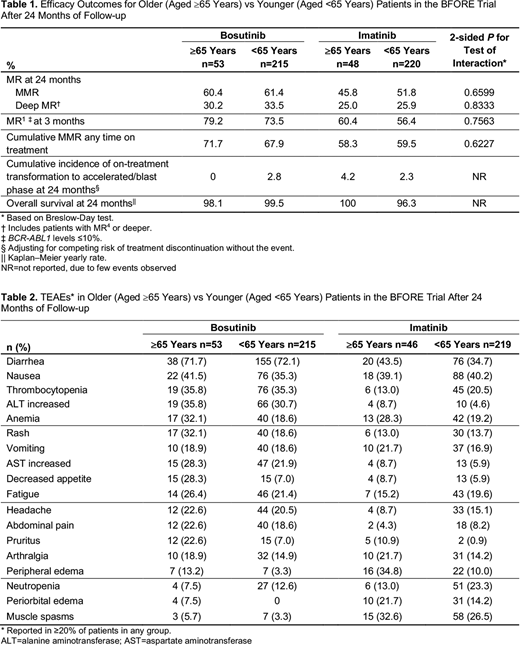
Results: In the bosutinib arm (n=268), 53 were older and 215 were younger patients. In the imatinib arm (n=268; 3 untreated), 48 (2 untreated) were older and 220 (1 untreated) were younger patients. Sokal risk scores were balanced between treatment arms but higher in the overall older (8.9% low, 70.3% intermediate, 20.8% high) vs younger (44.1% low, 34.7% intermediate, 21.1% high) populations, reflecting that age is part of the score. Bosutinib was discontinued in 32.1% of older and 28.4% of younger patients; the most common primary reason was treatment-related adverse events (AEs; 18.9% and 15.3%, respectively). Imatinib was discontinued in 32.6% of older and 33.8% of younger patients, most frequently due to suboptimal response or treatment failure (13.0% and 13.2%, respectively). The percentage of patients who discontinued treatment due to treatment-emergent AEs (TEAEs) was similar in the older vs younger group in both arms (bosutinib: 22.6% vs 19.1%; imatinib: 8.7% vs 12.3%). In older vs younger patients, median (range) duration of treatment was similar: 24.8 months (0.3-33.3) vs 24.9 months (0.3-33.5) for bosutinib and 25.6 months (2.9-33.1) vs 24.5 months (0.7-33.4) for imatinib. Median relative dose intensity was slightly lower in older vs younger patients in the bosutinib arm (92.8% vs 99.3%) but was 100% in both age groups in the imatinib arm. The difference in rates of major molecular response (MMR) at 12 months (primary endpoint) with bosutinib vs imatinib was consistent across age groups (older: 43.4% vs 35.4%; younger: 47.4% vs 36.4%; P=0.7879 for test of interaction), as was the difference in rates of CCyR by 12 months (older: 68.8% vs 69.0%; younger: 79.3% vs 65.8%; P=0.1689). MR rates at 24 months (and MR1 at 3 months) were generally similar in older vs younger patients within each arm and higher with bosutinib than with imatinib (Table 1). Time to achieve MMR on bosutinib was not different in older vs younger patients (hazard ratio: 1.227; P=0.2380, after adjustment for baseline and time-dependent covariates in a multivariable proportional subdistribution hazards model). Rates of common TEAEs in each treatment arm were similar (<10% difference) between age groups, except for higher rates of anemia, rash, and decreased appetite in older patients in the bosutinib arm; higher rate of pruritus in older patients in both arms; and higher rate of peripheral edema and lower rate of neutropenia in older patients in the imatinib arm (Table 2). In older vs younger patients in the bosutinib arm, there were higher rates of grade 3/4 TEAEs (75.5% vs 61.4%), serious TEAEs (39.6% vs 23.3%), and dose delays (69.8% vs 58.1%) and reductions (52.8% vs 37.2%) due to TEAEs. In older vs younger patients in the imatinib arm, rates of grade 3/4 TEAEs (43.5% vs 47.9%), and dose delays (39.1% vs 38.8%) and reductions (23.9% vs 21.5%) due to TEAEs were similar, but the rate of serious TEAEs was higher (28.3% vs 16.9%).
Conclusions: In the phase 3 BFORE trial, bosutinib showed clinical activity in older and younger patients with newly diagnosed CP CML. Difference in rates of MMR at 12 months for bosutinib vs imatinib was consistent in older and younger patients. MR rates at 24 months were similar in older and younger patients and higher with bosutinib than with imatinib. Although the incidence of grade 3/4 TEAEs, serious TEAEs, and dose modifications due to TEAEs were higher in older vs younger bosutinib-treated patients, treatment discontinuation rates were similar between age groups, suggesting that, regardless of patient age, TEAEs were manageable with bosutinib.
Deininger:Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Blueprint: Consultancy. Kota:Pfizer: Honoraria; Xcenda: Honoraria; Novartis: Honoraria; Incyte: Honoraria; BMS: Honoraria. Lipton:Pfizer: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding. Milojkovic:Incyte: Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; BMS: Honoraria, Speakers Bureau; Pfizer: Honoraria, Speakers Bureau. García Gutiérrez:Incyte: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; BMS: Honoraria, Research Funding; Novartis: Honoraria, Research Funding. Leip:Pfizer: Employment, Equity Ownership. Nick:Pfizer: Employment, Equity Ownership. Hochhaus:Takeda: Research Funding; Bristol-Myers Squibb: Research Funding; Novartis: Research Funding; Pfizer: Research Funding; Incyte: Research Funding. Gambacorti-Passerini:BMS: Consultancy; Pfizer: Consultancy, Honoraria, Research Funding. Cortes:Astellas Pharma: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Arog: Research Funding. Brummendorf:Merck: Consultancy; Pfizer: Consultancy, Research Funding; Janssen: Consultancy; Takeda: Consultancy; Novartis: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal